


Aspirin About-Face
Aspirin About-Face
A major reversal on aspirin highlights a concept everyone should understand


Welcome to Range Widely, the newsletter for generalists — where I'll help you step outside your lane for a few minutes each week.
****************************************************************
A whopping 29 million Americans — that’s the entire population of Texas — take aspirin every single day in order to prevent heart disease. Last week, the U.S. Preventive Services Task Force issued draft guidelines saying that most of those people should probably stop, because the potential harms outweigh the benefits.
That’s a big friggin’ deal. Medical recommendations change all the time, as knowledge is updated. But I think this case is a particularly teachable moment, highlighting the importance of comparing costs and benefits on the same scale. And there’s an important concept in medicine that can help with that — namely: NNT.
NNT is an abbreviation for “number needed to treat.” In other words: How many patients must be treated with the drug in order for a single patient to get the desired benefit?
When you read about drugs in the news — or even in most medical journals — you will almost never be explicitly given the NNT (which I will explain in more detail below). Instead, you’ll get relative risk reduction, a metric that a Michigan State med school dean once told me “is just another way of lying.” Why would he say that?
Relative Risk Reduction
Here’s a fictional example:
You read that a new drug reduces your chance of dying from Ryantastic syndrome by 40 percent. Here’s what that means in practice: if 10 in 100,000 people normally die from Ryantastic syndrome, and everyone takes the new drug, only 6 in 100,000 people will die from Ryantastic syndrome. Now let’s think about it from an NNT perspective.
For 100,000 patients who took the new drug, four deaths by Ryantastic syndrome were avoided, or one per 25,000 patients who took the drug. So the NNT is 25,000; that is, 25,000 patients must take the drug in order for one death-by-Ryantastic to be avoided. Ideally, you also want to know the NNH, or “number needed to harm.”
Let’s say that 1 in 1,000 patients who take the new drug suffer a particular grievous side effect. In that case, the NNH is 1,000, while the NNT is 25,000. Suddenly, the decision seems a lot more complicated than if you’re just told the drug will lower your chance of dying from Ryantastic syndrome by 40 percent.
Now let’s move to the real world: aspirin. Nearly five years ago, the NNT and NNH of aspirin caught my eye, so I included them in an article about medical evidence:
For elderly women who take it daily for a year to prevent a first heart attack, aspirin has an estimated NNT of 872 and an NNH of 436. That means if 1,000 elderly women take aspirin daily for a decade, 11 of them will avoid a heart attack; meanwhile, twice that many will suffer a major gastrointestinal bleeding event that would not have occurred if they hadn’t been taking aspirin.
And so why did the recent task force make the new recommendation? According to the New York times:
The U.S. task force wants to strongly discourage anyone 60 and older from starting a low-dose aspirin regimen, citing concerns about the age-related heightened risk for life-threatening bleeding.
They looked at the same kind of data that I did and saw that the tradeoff between the NNT and the NNH didn’t look so good. As a doctor I once interviewed on this topic told me: when a massive group of people who don’t have symptoms take a drug, the chances of harm will often outweigh the chances of help. That certainly is not to say that this is always the case, but as the old medical adage goes: it’s hard to make asymptomatic patients better.
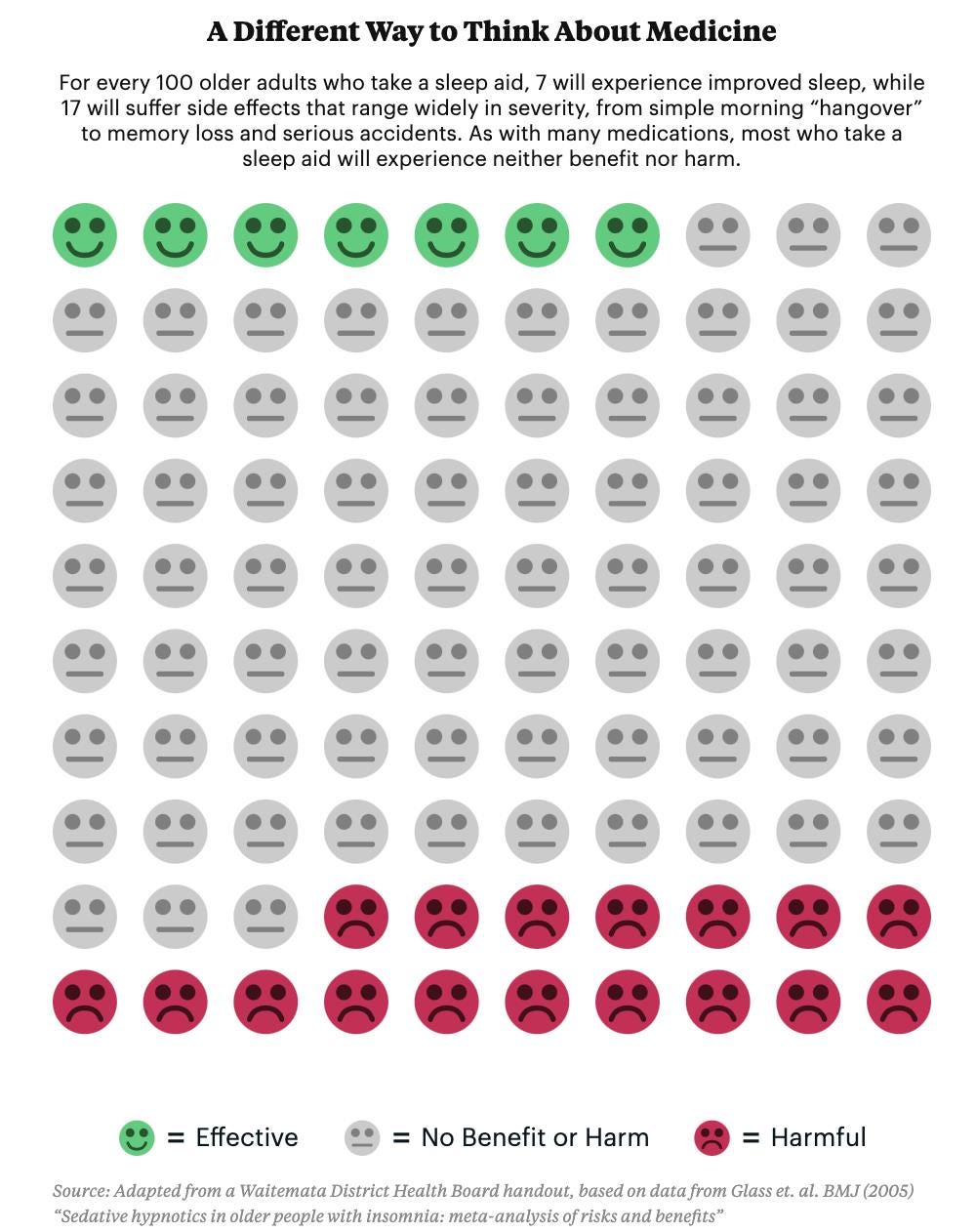
Once I started looking at NNT and NNH data instead of relative risk, one of my main takeaways was that most drugs don’t do anything significantly good or bad for most people who take them. That doesn’t mean they aren’t worthwhile, it’s just a different — and, I think, important — perspective. Here’s a graphic illustration of what I mean, from my 2017 ProPublica article:
WYSIATI: “What You See Is All There Is”
The larger point I really want to hammer home is that a statistic like relative risk reduction — which is far and away the most common one you’re getting — is not the statistic that you need in order to make an informed decision.
Daniel Kahneman, the psychologist who won a Nobel for illuminating cognitive biases, writes about a bias he calls WYSIATI, or, “What You See Is All There Is.” (Pronounced <wiz-E-ah-tee>.) In his words:
WYSIATI means that we use the information we have as if it is the only information. We don't spend much time saying, "Well, there is much we don't know." We make do with what we do know. And that concept is very central to the functioning of our mind.
The question we should ask: Here is the information that I was given; is it the information that I need in order to make a good decision?
A few years ago, I sat in on several days of a Harvard Business School class taught by Max Bazerman. (I was blown away by how engaging he was. I watched him auction off a $100 bill to HBS students for nearly $500. It was bananas.) Over the course of a two-day simulation, Bazerman showed students that they were making serious business decisions based on the information he had given them, but without asking for the information they actually needed.
On day one, he repeatedly told the students they could contact him after class if they wanted more information. When they returned on day two, Bazerman asked the class: “How many times did I say yesterday, ‘If you want additional information let me know?’” And then he answered himself. “Four times. Four times I said, ‘If you want additional information, let me know.’” Not a single student had asked for additional information.
After most of the students realized that they had botched the business decision in the simulation, Bazerman continued:
If I was in your situation I would probably say, ‘but in a classroom the teacher typically gives us the material we’re supposed to have,’ but I would highlight that it’s often the case where you’ve been in group meetings where the person who made the PowerPoint slides — me in this case — often puts data in front of you and I would argue we don’t do a good job of saying, ‘Is this the data that we actually want to make the decision that we want to make?’ We often use the data that people put in front of us rather than ask them that particular set of questions.
How I Apply This
When I have a major decision coming up, I try to make a quick list of the information I would want in order to feel informed. And I try to do this as early as possible, so that when I’m presented with information, I can see if something from my list is missing. (I did this recently while considering a home purchase, and found it very helpful.) It’s not perfect, of course, but I think it keeps me seeking out useful information, and helps me avoid falling prey to WYSIATI. Give it a try!

David’s Digressions
-If you’re interested in checking out NNTs for other therapies, check out The NNT, a site staffed by volunteer doctors. If you click “reviews,” and then over on the left sort by “rating,” you can check out therapies that are rated green — like defibrillators for cardiac arrest, or chewing gum after a C-section — and those that are red, like a drug that has an NNT of infinity for a given condition because it doesn’t help anyone. Some therapies that get the “Black/Caution” rating might surprise you, like vitamin D supplementation for preventing fractures in older adults.
-If you want to read more about “medical reversals” — i.e. U-turns of medical advice — the book Ending Medical Reversal has some fascinating examples, as well as suggestions for making reversals less common. More recently, two of the same authors suggested an “expiration date” by which medical evidence should be reevaluated. Of course, reevaluating in light of recent evidence is exactly what the task force that drafted the new aspirin guidelines did. So while millions of people who have been taking aspirin daily on the advice of their doctor might be upset and confused by the new recommendation, I think we ought to celebrate an effort that updated our thinking. I’m sure leaving the status quo alone would have been the path of least resistance, so kudos to the task force.
Thanks for reading. Until next week…
David
p.s. If you liked today’s post, please share it!
Thank you. I had never heard of NNT or NNH, but I used the same concept (though less clearly) in my essay on Carbon Dioxide http://frank-hood.com/2022/09/24/to-warm-or-not-to-warm/
"Like the TV commercials where they warn you that eating too many hamburgers might double your risk of getting cranial-rectal cancer (from 1 in 10 million to 2 in 10 million they neglect to say), they don’t lie exactly, they just make something sound like a big deal that might not be such a big deal. "